
Gunshot wounds are becoming more common at demonstrations. This is not to say you should panic—millions of people have participated in demonstrations over the past four months, while only dozens have been shot. Still, as political conflict escalates in the United States, it is important to think about how we can care for and protect each other. The good news is that even if you have no medical training, there are things you can do to maximize the likelihood that a person who is shot in your vicinity will survive—simple things like learning the location of the nearest trauma center. Though this subject can be stressful to contemplate, the following guide may equip you to help save lives.
While many demonstrators have learned how to prepare for tear gas, pepper spray, rubber bullets, LRADs, baton blows, and arrests, few are currently prepared to respond to gunshot wounds. This guide is drawn from the experiences of several people who have witnessed or treated gunshot wounds in the course of political and social conflict. In order to demystify the subject and help readers imagine how they might employ this information, we’ve included two personal narratives describing experiences with gunshot wounds at demonstrations.
Although this text draws on the practical knowledge of a number of people with both institutional training and street experience, it does not represent professional medical advice. It includes some information that will chiefly be useful to experienced street medics, but most of it is relevant to any reader. It is not intended to stand in for actual training in gunshot wound response or other medical interventions. We encourage readers to seek out additional training, skills, and life-saving critical response tools.
What Is a Gunshot Wound?
Gunshot wounds involve traumatic injuries and serious puncture wounds. Their impact on the body varies according to the type of weapon, the distance of the shooter, and the location of the entry wound. Depending on the size and speed of the bullet, gunshots can inflict different types of harm—including severe bleeding, muscle and bone damage, and destruction of organs. They can damage bodies in unpredictable ways.
While some calibers of ammunition may pass directly through a person leaving easily identifiable entry and exit wounds, other calibers are more prone to “tumbling,” or ricocheting, inside the body. This can cause more internal damage and less predictable exits. Worse still, some types of “self-defense” ammunition for handguns are designed to “mushroom” out on impact, causing severe harm.
Treat any gunshot wound as a potentially life-threatening injury, regardless of the details. If an artery is compromised, a person can bleed out in as few as three minutes. Once a person loses half their blood, their chances of survival decrease dramatically. It is up to you to act quickly.

Pay Attention
First and foremost, pay attention to what is going on around you. Street demonstrations can be chaotic and loud. Police may employ tear gas, flash-bang grenades, LRADs, and other noisy weaponry, while protestors sometimes set off fireworks—which can sound an awful lot like gunfire. When you are surprised by loud bangs in the streets, try to identify the source and what kind of risk it represents.
Stay aware of the location of anyone who is openly carrying a firearm, as well as anyone you have reason to believe may be carrying a concealed weapon. People have been hit by friendly fire at demonstrations as well as hostile fire. If you are working with an affinity group, you could designate one person to keep an eye out for potential threats. Take turns occupying this role, so one person doesn’t become exhausted from being constantly vigilant. In any case, all parties should stay aware, as things can shift rapidly.
Communicate clearly and concisely, especially when you are describing individuals with firearms. This can help others to make wise decisions rapidly in an emergency, without contributing to undue panic. Here are two communication models you can employ to convey what you see.
Use the mnemonic device “S.A.L.U.T.E.” (Size, Activity, Location, Unit, Time, Equipment) to identify potential threats. For example, rather than shouting “They’ve got a gun!” you might report, “I saw three men (S) guarding the convenience store (A) at the intersection of Main Street and City Avenue (L). Possibly militia (U). This was at 11:15 pm (T). Two had long guns, I don’t know about the third (E).”
In emergencies, or when time is of the essence, you can use another tool called the “three Ds”: Direction, Distance, Disposition. For example, “Four unknown white men with rifles at my 1 o’clock, one block up, scanning the crowd with binoculars.”
Be Prepared
Much of what you can do to treat a gunshot wound takes place long before the shot is fired.
Street Medics
Depending on the type of event and where it is taking place, there may be medics around. You could investigate in advance whether there are street medics in your area, whether they will be attending, and where they will be positioned. During demonstrations, one often sees medics milling around in the crowd or stationed at the margins, carrying gear and wearing a red cross or a similar insignia identifying them as medics. If you believe it could become relevant, you can ask them whether they are prepared to deal with gunshot wounds and other severe injuries. Many medics have experience responding to tear gas, pepper spray, and rubber bullets, as well as exhaustion, dehydration, and panic. Currently, it is less likely that a medic who responds to a gunshot wound will possess the relevant skills and experience.
If you are assessing the extent to which local medics are trained to deal with gunshot wounds and you learn that they are prepared to offer “first response” care, you can also inquire as to whether they have the capacity to offer prolonged care in the event that EMS services cannot reach an area. This can give you vital information about the potential risks you may be taking on if you remain in an escalating situation.

Street medics in the Bush era.
Before the Demonstration
Before going to a demonstration, assess the security and health needs of your comrades—including ability and willingness to call for emergency services, which are usually accompanied by police. Are there any needs that should be addressed before someone reaches the emergency room? Who would you like your friends to contact first in the event of an emergency or injury?
In addition to learning whether trained medics will be around, make sure you know the location of the nearest emergency room—preferably one with a trauma center. Not all hospitals are equipped to deal with life-threatening wounds. If you will not be near a hospital with a trauma center, at least learn the location of the nearest hospital. With any luck, they should be able to stabilize a victim before transferring them to a hospital that is prepared to deal with mass physical trauma.
Equipment
There are several items you can carry with you that can be useful in the event of a shooting. Consider procuring or building an Individual First Aid Kit (IFAK) to carry with you. An IFAK is a trauma kit containing essential life-saving materials to help you control bleeding and treat major wounds. It is usually a small pouch containing items such as a gauze (regular or hemostatic), pressure dressing, personal protective equipment (gloves, face shield), and a tourniquet. An experienced medic has compiled a thorough list of what to put in an IFAK and where to obtain it, which is included in an appendix below. With the exception of PPE, which protects you and the person you are assisting from blood-borne pathogens or other communicable diseases, all of these intervention tools share the same purpose: to stop bleeding as quickly as possible.
Gauze is a basic part of an IFAK, but a crucial one. It is used to absorb blood as you apply direct pressure to a wound. It can also be used to “pack” inside of a larger wound.1 Hemostatic gauze (often known by brand names such as QuickClot, Celox, and Hemcon) is gauze impregnated with a mineral agent that helps blood clot more quickly, which is critical in the case of a major bleed.
A pressure dressing (also referred to as an Israeli bandage, emergency bandage, or emergency trauma dressing) is an elastic wrap, similar to an ace bandage, with an attached non-adherent absorption pad and a Velcro or clip closure system. When holding pressure on the wound with your hands is not enough stop the bleed, a pressure bandage is used to apply stronger, constant pressure to a wound. There are many different models of pressure dressings; if you carry one, make sure you know exactly how it works. Online training or gear review videos are great for this.
A tourniquet is the cornerstone of an IFAK. If you carry only one intervention tool, invest in a quality tourniquet. When purchasing a tourniquet, it is ideal to acquire one approved by the Committee of Tactical Combat Casualty Care. These tourniquets have undergone rigorous pre-manufacturing testing and have been thoroughly vetted through field use. We recommend a CAT-7 Tourniquet. One can cost around $35; you and your comrades may be able to buy them in bulk to save money. Beware of fakes! Many cheaper versions are in circulation; these can fail under pressure. You can usually recognize a fake by the absence of a factory stamp by the red pull tab; a skinny windlass (i.e., the rotating rod) can also be a giveaway, instead of a beefier one with extrusions. Finally, and most obviously, no black CATs produced before 2009 have white “time” straps. Fakes notoriously have these white straps.

The one on the top is a cheap knockoff that could fail under pressure.

The one on the right is a cheap knockoff that could fail under pressure.
It is good practice to keep your tourniquet with the band already threaded through the buckle, creating a large loop you will then pass over the foot or hand, rather than attempting to thread the buckle in the heat of the moment if you need to use it.
Finally, carry sharpies to mark the time that a tourniquet was applied or any additional information that first responders—street medics or otherwise—may need to know. Black sharpies work for white people or lighter-skinned people of color, while silver sharpies work better for Black comrades.
Even if there is a trained and experienced medic collective local to you, carrying an IFAK, or even just a tourniquet, is a great idea. In the scope of emergency casualty care, many properly trained medics will seek to use the injured comrade’s equipment on them first, in order to save their specialized equipment for those who did not carry anything. Because of this, be sure to mark your IFAK or blowout kit clearly and carry it somewhere that is easily accessible. Failing this, make sure to have your tourniquet easily accessible, in a marked, visible location that is known to everyone in your affinity group. Normalize the practice of letting your trusted comrades know where your medical equipment is located.
If a Shooting Occurs
Several things can happen in the immediate aftermath of a shooting. If police are nearby and intervene, it is possible that you will rapidly lose control of the situation. Despite their general lack of medical training, they will typically form a cordon around the victim and prevent a medic or anyone else from treating them. This does not necessarily mean they will act quickly in response to the injury. Put pressure on the police if they aren’t doing enough, or doing it fast enough. Demand they seek proper medical care for the injured.
https://twitter.com/crimethinc/status/1300285181530640391
The flip side of the scenario is just as possible—you and your comrades may have to make do without state intervention. If the situation is chaotic or deemed dangerous, even if you are willing to call emergency services, an ambulance may not enter an area. Police may spend an inordinate amount of time trying to clear the area with tear gas or other means before they bring in an ambulance—they might even simply prevent an ambulance from reaching you. In such a situation, depending on the severity of the wound, survival may depend on quick thinking and action. In that case, you will have no one to depend on except yourselves to care for the wounded and organize your evacuation.
Continually assess what’s going on around you. Are there still gunshots being fired? Is there traffic in the area? Are people running past you fleeing from a shooter, police, or fascists? Don’t let panic, haste, or inattentiveness cause additional misfortunes.

A small Individual First Aid Kit (IFAK) containing a tourniquet and trauma dressings.
Immediate Treatment Options
Nothing you could read here can substitute for proper medical training. However, if you own an IFAK or tourniquet and possess a basic understanding of how to stop a bleed on an arm or leg, some action may be better than nothing.
If gunshots ring out, try not to panic. First, get to a safer place. In the system of Tactical Emergency Casualty Care, the first step is to maintain scene safety, so you do not become a casualty as well. Find cover from which to assess the situation. “Cover” designates anything that can stop the rounds you are facing, which depends on the situation and the caliber of weapon. Consider a brick wall or the engine block of a car.
If you determine that someone has been shot and you are equipped to provide aid, make sure the scene is relatively secure. If you can determine this, communicate to your friends that you intend to move to the person who has been hit. While moving, ask the person questions to determine how to care for them: “Where were you shot?” or simply, “What is your name?” If they answer these questions before you reach them, this will indicate that their airway is open and they are conscious, and you may obtain enough information to start preparing your equipment and mindset.
Your first thought will likely be, “That’s a lot of blood!” Initially, you may have a difficult time identifying exactly where the wound is, especially if the individual is wearing long-sleeved dark clothing. Quickly expose the injury, using trauma shears (special scissors designed to cut quickly through clothing) if you have them. In general, it is important to expose an injury at skin layer to understand the exact scope and extent of the wound.
Immediately apply direct pressure to the wound. Ideally, you would use a gloved hand and a gauze pad (preferably hemostatic gauze), but in an emergency, you can use a t-shirt, scarf, or extra mask. If blood soaks through the gauze, add more gauze or another cloth layer and apply more pressure. If holding direct pressure with your hands does not stop the bleeding, apply a pressure dressing. Place the sterile absorption pad over the wound, and over any gauze that has already been applied (never remove gauze—this could disrupt any clotting that may have started). Wrap the elastic bandage firmly around the injured part of the body. It should apply a lot of pressure, but not enough to cut off circulation.
With a life-threatening bleed, time is of the essence. If the wound is clearly on an arm or a leg and you can see a lot of blood, you may choose to apply a tourniquet immediately. Unlike holding direct pressure with gauze or using a pressure dressing, which stops bleeding from a specific wound, a tourniquet cuts off all distal circulation to the limb, meaning that it should stop all bleeding that is further away from center body than where the tourniquet has been applied. If applying a tourniquet over clothes, quickly check to ensure that you are not fitting it over items in a pocket or anything else that could obstruct the pressure.
Many people have been taught that using a tourniquet is likely to result in the loss of the patient’s limb, due to complications from cutting off circulation; in fact, this is still commonly taught within many wilderness/remote medicine and street medic frameworks. Data garnered from combat zones across the globe, however, has shifted the understanding of tourniquet safety. Certified tourniquets such as the CAT-7 are now understood to be highly effective and safe live-saving devices, rarely resulting in long-term damage or side effects. Used correctly, they are considered an appropriate first line of intervention, rather than solely as a “last resort.” As the everyday demonstrator’s threat model changes—especially if the streets increasingly take on the contours of a combat zone—models of intervention based on armed conflict scenarios, such as the Tactical Combat Casualty Care framework, will gain increasing relevance.
For a succinct step-by-step guide to using a tourniquet, see Appendix III.
To apply a tourniquet, open your CAT-7 and make sure that the band is passed through the single routing buckle and the red tip is pointed towards the heart. Then slide the tourniquet up the extremity as high as you can possibly go, while taking the individual’s genitals into consideration if applicable. If the wound is clearly below the knee or elbow, and you can easily see there are no wounds higher on that limb, you can place the tourniquet just above those joints. Once you have it in position, make sure the strap is as tight as you can make it—think “ratchet strap.” If you can stick even one of your fingers beneath the strap, it is not tight enough. Turn the windlass until the flow of blood stops. Pull the “strap” closed through the windlass clip and mark the time applied on the time strap. This process will hurt your comrade immensely, though likely less than the initial wound, depending on its location. Talk to them while you are applying the tourniquet and afterwards as you are able.
Prior to ever using a tourniquet, you should get a sense of how tight it has to be to be effective. Try placing it on yourself briefly just above the elbow before the demonstration and tightening it until you no longer feel the pulse at your wrist. This is a good exercise in empathy, to know what kind of experience a person you treat will endure. Never leave a tourniquet in place for more than a few seconds except when treating an actual wound.
As soon as you have stopped the bleeding—by using direct pressure, a pressure dressing, or a tourniquet—immediately being to look for other wounds. Sweep underneath all parts of the body with gloved hands. Check your hands for blood regularly during the sweep so you can immediately identify which part of the body is injured. If the injured person is wearing waterproof clothing, make sure to remove or sweep inside of those layers, as a rain jacket or rain pants can keep blood next to the body, concealing a major bleed. Do not wait to apply a tourniquet if you find a major bleed on an arm or leg. Pause the sweep, apply direct pressure, a pressure dressing, or a tourniquet, and resume sweeping once that bleed is controlled.
Bleeds that are in junctional areas (i.e., the groin proximal to the inguinal ligament, the buttocks, the gluteal and pelvic areas, the area under where the arm connects to the shoulder, the shoulder girdle, and the base of the neck) can be controlled by “packing” the wound, which applies direct pressure to the severed artery or vein. If you are in an unsafe area, or if you are not equipped with wound packing material, direct pressure on the wound, ideally with a gauze pad, can do for the time being.
If you are not equipped with an IFAK or tourniquet, call loudly for a medic. Call out landmarks to guide them quickly to you, as well as crucial information such as whether the casualty is bleeding considerably: for example, “I need a medic! I’m behind the red sedan—someone has been shot in the leg!”
While you wait for them to arrive, use direct pressure to slow the bleeding. If the bleed is capillary (slow and even flow, bright red in color) or venous (steady flow, dark red in color), you may be able to control the bleed with direct pressure. If the bleed is arterial (spurting or pulsing flow, bright red in color), direct pressure won’t be enough—you will have to apply pressure at an arterial pressure point. If the wound is in the leg, consider applying pressure in the upper thigh, near the pelvic region—but be careful. If there is a wound in this area, try applying pressure in the lower right abdomen. If the wound is in the arm, try applying pressure underneath the armpit. If the bleeding is on the neck, try applying pressure on the side of the neck generally underneath the point of the jawline, keeping in mind to apply pressure only on one side. Only do this in an extreme emergency, as it is of limited value for bleed control.
Regardless of where the wound is, once you apply pressure, do not remove pressure to check if the wound is still bleeding. Continue to apply pressure until a medic can place a pressure dressing or other hemostatic intervention.
If the wound is in the chest, it is acceptable to cover the wound with your gloved hand, but applying too much pressure can potentially inhibit their respiratory system. Chest wounds generally present with less bleeding, but run a high risk of air entering the chest cavity, leading to a buildup of pressure that can cause a lung to collapse. Some medics carry vented chest seals in their kits, which serve the same general purpose as a gloved hand over the wound: preventing air from entering the chest cavity. If the wound is in the trunk—i.e., between the chest and the navel—there is probably little you can do to help besides notifying a medic or other higher care immediately.
If you can control the bleed, you or a friend should prepare the victim for a possible ER visit or another situation in which they may have their possessions confiscated. Remove any potentially incriminating items from their backpack, pockets, and person. Dispose of these or give them to a trusted friend who can remove them from the scene.
When higher care arrives, whether that is EMS or street medics, give them a report to the best of your ability, using the MIST acronym: the Mechanism of injury (M), the Injuries sustained (I), the Symptoms (S), and any Treatments (T) given. For example, “They were shot with a rifle from about two blocks away, they received two bullet wounds in their left leg. Their skin is cool to the touch, and their breathing seems slower than normal. I applied a tourniquet high and tight and the bleeding seems to have stopped.”
If it takes a while for medical care to arrive, consider writing symptoms or other things you notice on the patient’s arm with your marker.

A small IFAK that can be worn on a belt, marked with a cross for easy identification.
Evacuation
Know your options for evacuation. Are you behind a police line that an ambulance cannot pass through? Does the local medic collective offer transport to hospitals? You can try calling for an ambulance if you think you are in an area they can enter. When you place a 911 call for an ambulance, you can request that they do not send police in tandem, but they may well ignore your request. If you do decide to call EMS while you are in a group actively trying to assist someone who has been wounded, designate one person to make the 911 call and report the wound and location while the rest of you stay focused on assisting the victim. It is possible—but not guaranteed—that a 911 dispatcher can walk you through basic trauma response until you receive help or can transport the wounded.
If you or your comrades have driven to the demonstration, it can help if a car is parked nearby with immediate access to the road. Make sure the location of the keys is known and accessible to more than one person. Other people will likely wish to assist in the event of a shooting. If you cannot transport the patient yourself, seek aid from those around you.
At the Hospital
In some cities, hospitals place shooting victims in protective custody to eliminate the threat of violence against them.2 If that occurs, you will not be able to locate your friend inside the hospital system. If the person is unconscious and unable to tell healthcare workers who to contact, the workers will try to contact a family member. If you are entering a situation in which it is possible that you will be severely injured, you could write an emergency number in sharpie on your skin with the instruction “call in case of emergency.”
While this may not be uppermost in your thoughts in the event of a shooting, it is important to know that most large hospital systems offer programs via which you can apply for aid to reduce or forgive your bills. If someone’s life is on the line, you can work out the financial details later.
Back at Home
When bringing someone home from the hospital, evaluate their home situation. Do they live alone? With friends or family? Is their bedroom up a flight of stairs? Depending on the severity of the injury and the forecasted length of their recovery, they may need to change their living situation.
Because there is very little semblance of a public health system in this country, people are often released from the hospital very rapidly—sometimes before they are ready to go home. This can be intimidating, but the good news is that home is usually a better recovery environment than an institution. You can rent a hospital bed from a hospital or home-care equipment rental company—they are surprisingly inexpensive and can be enormously helpful in the case of a long-term recovery.
If necessary, organize community care so people are present or available around the clock. Even if that is not necessary, try to organize a caregiver schedule involving a rotating cast of friends and loved ones to ensure that care does not fall solely or mostly on a partner. In addition, you can create a meal schedule for people to drop off food and groceries or cook for the wounded and the caregivers.
Trauma
While it should go without being said, being shot—or responding to someone getting shot, or witnessing someone getting shot, or having someone you love get shot even if you weren’t there—is a traumatic event. You may experience a range of responses including nightmares, anxiety, flight/freeze/fight responses, self doubt, jumpiness, fear, and depression. Seek help! Form a community care circle and meet weekly to process the pain, confusion, and trauma.
If many people in your community were affected by the event, you can seek out a friend or loved one from outside your circle to help you process what happened. Find a therapist in your town to help you work through your feelings. While therapy can often seem cost prohibitive, there may be a non-profit, a clinic system, or a university where counselors in training can offer services for free or a reduced price. If there are ongoing protests in your city, local non-profits may offer counseling specifically for those affected. This guide written in response to the COVID-19 pandemic offers some tools you can apply to coping with trauma.
There has been a longstanding tendency in anarchist milieus to emulate tough attitudes and bravado. Analyzing and overcoming these cultural norms and eschewing a dichotomy between “passivity” and “militancy” can help us to build sustainable long-term movements. Remember, we want a thoroughgoing social revolution, not just periodic street violence.
In the Context of a Long-Term Struggle for Liberation
There is a long history of state-sanctioned violence in the United States, against both ordinary people and movements for social change. Alongside this extends an equally long history of extra-state violence, from the lynchings of the not-so-distant past to contemporary equivalents like the murders of Trayvon Martin and Ahmaud Arbery. Since before the American Revolution, extra-state forces have worked in tandem with the state to uphold patriarchal white supremacy. It is well documented that police continue to cooperate with white supremacists. They are two sides of the same coin.
The current clashes between white supremacists and anti-fascists are reminiscent of the rise of Nazism in Germany. In the early 1930s, when the Reichstag election campaigns were in full swing, fascists repeatedly baited their adversaries into street fights, injuring many while framing themselves as “victims in a lawless country.” They used this violence to bolster their campaign for “law and order,” a pretext to impose a dictatorship. Sound familiar?
There have now been many instances of lethal violence during demonstrations, including the murders of Heather Heyer in Charlottesville, David McAtee in Louisville, Garrett Foster in Austin, and Anthony Huber and Joseph Rosenbaum in Kenosha. It is vital that we learn how to navigate these increasingly violent and contested spaces. If we are to sustain a culture of resistance, we’ll have to be prepared to respond to a wide array of scenarios. We can learn to deal with violence and mitigate its effects while refusing to glorify or romanticize it.
As social conflict deepens, more and more people are becoming familiar with the violence that the state has long meted out overseas and against Black and Indigenous communities inside the United States. This must not deter us from action—it is better for us to confront these threats together, head on, than to try to hide from them until they reach each of us in isolation. Generalizing care and aid is an essential part of staying safer in the streets, which, in turn, is part of creating safer communities and, ultimately, a safer world for all of us.
As frightening as this situation is, you are not alone. The same dynamics that are destabilizing our lives and our society offer us the opportunity to connect with each other and reinvent our lives on a new basis. Thank you for everything you have done to become part of the momentum towards a better world.

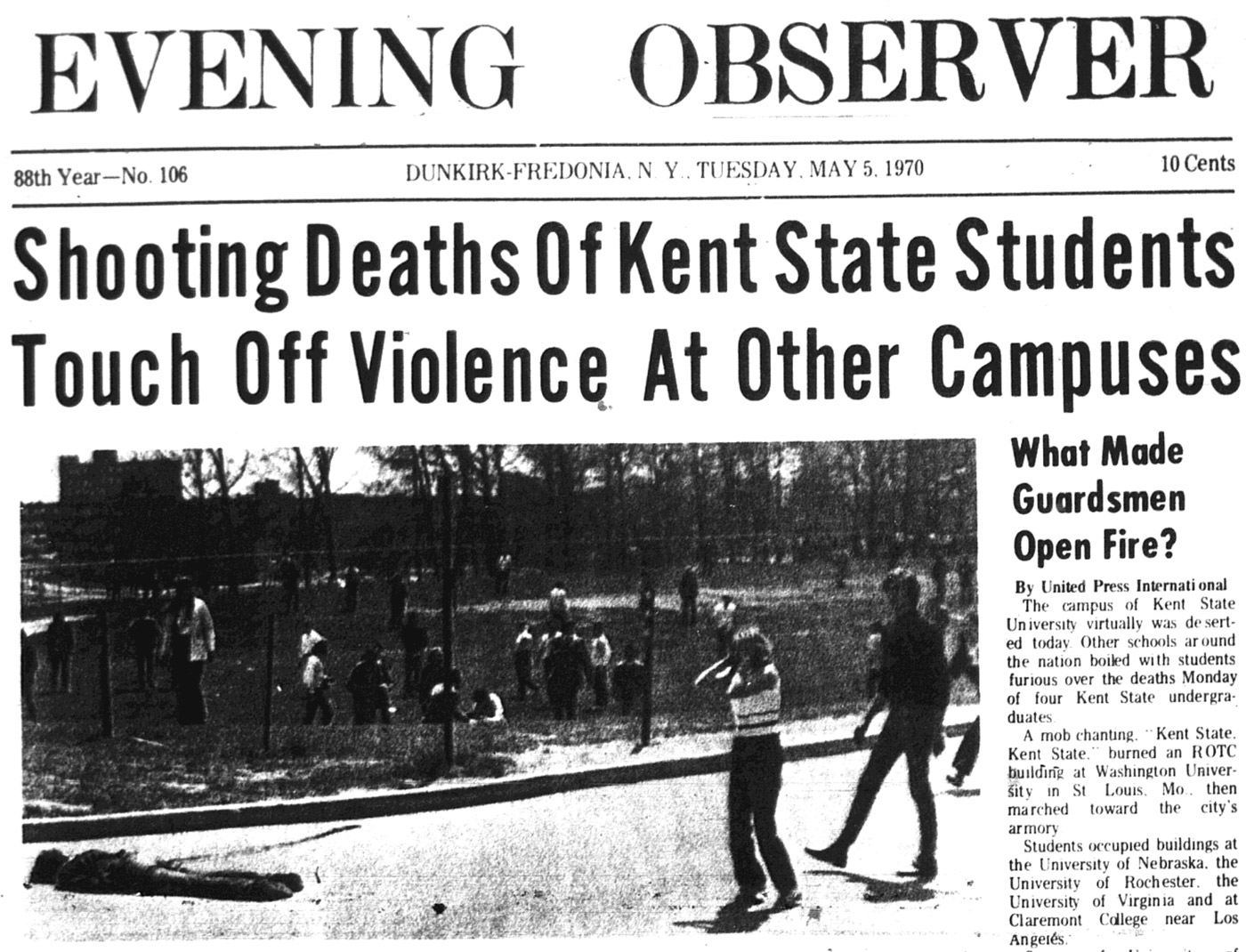
On May 15, 1970, policemen in riot gear fired more than a hundred and fifty rounds in twenty-eight seconds, murdering two young Black men at Jackson State campus in Mississippi and injuring a dozen more. While the murders at Kent State a few days earlier remain widely known, the subsequent murders of young Black demonstrators in Jackson and Augusta, Georgia are often forgotten.
Appendix I: Personal Narratives
The following accounts may help you to visualize how you would conduct yourself in similar circumstances.
The Line between Life and Death
It is a dark and stormy night, the first night it has rained all week. People are milling around under the awning of a barbecue joint, hanging back from the police line, waiting to see what will happen. More than a few folks have guns tucked in their waistbands. Some people scuffle with the police, some break up chunks of concrete to throw at the tanks; others listen to heated arguments about whether we should go home, stop violating the curfew, and leave the fight for another day. Then, out of the blue, a lone cop car comes squealing in from behind, sirens blaring.
The crowd scatters, people panic, running in all directions, as tear gas canisters skitter across the street and flash-bang grenades explode from the police lines. Choking smoke and chaos and fear everywhere. Gunshots ring out as people fire through the crowd at the lone cruiser, which has turned around to retreat. I dive to the ground by a blue mailbox, confused and separated from my friends. A tide of people flows down the street away from the police lines, as the cops start to push the crowd forward, hoping to clear it. Swept up in the sea of people, I take perhaps twenty steps down the sidewalk before I come upon a knot of people gathered around a figure on the ground.
Time slows down. Two of my close friends are clustered around a body on the sidewalk. That body is one of my oldest and dearest friends. Someone is screaming, “He’s been shot, he’s been shot!” One of my friends is shouting for people to back up, pushing people back, when he looks up and sees me. I look from him to my friend on the ground, who has been shot in the leg. But the light is fading in his eyes as he clutches his torso and moans. Getting shot in the leg isn’t enough of an explanation as to why my friend is crashing. We’re so confused—there’s no blood, there’s no blood. What the fuck happened? Where else is he hurt? There’s no blood, just a stumbling, haunting groan from his mouth. I am a mother, I have birthed a small person into this world. I know what it sounds like at the line between life and death, and all I know in this moment of despair and confusion is that this person I love so much is straddling that line before my eyes.
I still don’t know what the fuck is happening, but I do know that we have to get him out of there ASAP. No one is coming to help us and no one is coming to save him. I run to my car—thank goodness I parked only a few blocks away. I speed around screeching cars that are doing donuts in the street. When I get back, I find people lifting my friend’s body into an already packed car. I scream and scream that he is coming with me as my friends wrest his body away from the well-intentioned strangers. We race down the street into a rabbit warren of loopy suburban streets. I know what hospital I want to go to, but it’s dark and I’m confused. Riot angels pull up next to us and ask if we need to be led to the hospital.
When we arrive at the hospital and pull my friend from the car, his shirt slides up and there it is: an entry wound with no exit wound. He is immediately transferred to a trauma hospital. Over the following days, we hear over and over the words “should have died.”
Before this, I didn’t know that I didn’t know what it meant to get shot. What getting shot means is that a bullet rips through muscle, maybe through bone, maybe destroys some organs—quite possibly some that are essential. It could destroy the left kidney or the spleen; it could collapse both lungs, clip the esophagus, fill up the inner cavities with blood as the body bleeds out internally. A bullet could end up in the heart. You could find yourself in a hospital in the middle of the night, being coaxed through a series of legal documents by a very patient and very kind cardiologist who is preparing to do a second open heart surgery on someone you love to fish out the bullet that is lodged in his heart.
Luck was on our side that night, absolutely. But we responded to the situation quickly. I found out later that many different friends had passed by, that I wasn’t the only one running for a car—I just got there first. And well-intentioned strangers were trying to evacuate my friend on their own—so many people get shot in this city that people recognized what they were looking at and how important it was to respond.
What happened to my friend hasn’t stopped me from returning to the streets, and it hasn’t stopped him or other people in my community. Because the hospital placed my friend in protective custody, only one other friend and I could be there with him. Many of my friends sought comfort in the street battles that continued to rage, glad to have an opportunity to turn their grief, fear, despair, and anger into action.
I’m thankful that I happened to be parked close that night. I’m thankful that so many people around us wanted to help. I’m so thankful that people realized we needed them to lead us to the hospital. I’m thankful that the transfer to the trauma center happened quickly enough and I’m thankful for adept and willing surgeons. I’m thankful that my friend’s inner will was strong enough that he survived. I’m so thankful he lived. I’m thankful that there are things you can all do, too, to make it likely that things will turn out as well as possible if you ever find yourself in a similar situation.
And I am thankful for riot angels. May they be by your side if you ever need them.
A Single Pop
We all heard it. A single pop. It rang through the night, oddly out of place after hours and hours of hushed scuffles and the rustling of an agitated crowd. Hundreds of people were in the square—many lined up to get inside the event, and possibly an equal number trying to stop them. Red hats sailed above the crowd like short-range fireworks as people snatched and threw them. It was a mess, the conflicts impossible to follow; eggs, paint bombs, pepper spray, and punches coming at odd angles and from all directions. The few police that were on hand didn’t intervene. Stepping back from the square into the dark campus streets, the entire situation looked like a poorly directed fight scene in a low budget play.
But we all heard the pop. Just the one. Instinctively, the black-clad crowd dispersed throughout, the red hats all looked up. Given our knowledge up to that point of what happens at demonstrations, we assumed it was a flash-bang grenade. That was the only thing we thought could make that noise. But there was no second bang. Everyone’s eyes refocused on the stalemate around them. Pushing and shoving, some reinforced banners and phones being snatched, but a relative calm.
Looking up across the square, I caught a glimpse of something out of place. It was someone I recognized, someone I knew was in trouble. He had been trying to ensure that no one would get hurt, mixing distraction and de-escalation. Now something was wrong, but it was impossible to tell what it was.
A comrade and I pushed our way through the crowd to where he was. To get there, I walked through something hanging in the air—my brain wouldn’t put it all together for a while. It wasn’t a smell, it was more of a taste, a cloud in the air that had a tang of metal. Once we reached him, the look on his face told me that I was in over my head. That, and the sound. He was making a sound that you just don’t make. A scream and a gurgle mixed into one. I don’t know how he was still standing. I got to him first and he leaned into me, all dead weight. The smell of his leather jacket and the press of him onto my smaller frame in that moment of desperation is one of the things that would enter my dreams and wake me for years after. It was as if I was carrying a dead but still living body.
He stared right at me, but looking past me. I realized he was dying. But I had no idea why. Reasons flashed through my head; there was almost no blood and I couldn’t find anything. We didn’t walk that far—twenty feet at very most—and the best I could come up with was that he must have hit his head, only a head injury would make him incoherent like that.
And then as quickly as I had taken his weight, the medics took him. His weight left mine and we were uncoupled from that moment. I stared at the medic, who I thankfully trusted, and all I could get out was “He’s hurt, I don’t know,” or something like that. Besides walking him out of the danger of the immediate moment, I felt totally useless. The medics began doing their part, on the ground where there was a fair amount of blood now, trying to run through what their training had taught them. I heard the crowd as a low din—that thing that happens when you’re about to pass out and the audio goes to the end of a tunnel. But that was when I finally put it together: pop, metal, gurgle.
Someone had shot him.
The police swooped in and took him, pulling the trained trauma medics away by force as we all screamed from the other side of a police line. Now everyone knew he was dying, that something had gone wrong. I wanted to scream that he had been shot; I started to, but then I realized that it might cause people to panic. I was just barely aware that I was already panicking. I found one of the medics; they confirmed that someone had shot him.
The police loaded him into the back of some kind of open-air vehicle—campus cops with a golf cart. And the demonstration continued. I panicked openly at that point, finding my crew and demanding that we leave, that “they” were shooting at us and we had to go. But at that point, I didn’t even know where the threat was coming from or if leaving was safer. So we pushed back along the line of people trying to see Milo talk, well after the event had been closed off. The police never moved in, the “active shooter on campus” alert was never activated, and we stayed in that crime scene—for hours.
Appendix II: Additional Resources
Live Like the World is Dying podcast recently aired an interview with an experienced street medic who gives detailed instructions about responding to gunshot wounds at demonstrations.
In this podcast, Hex, who survived a shooting attack by a fascist at a demonstration on January 20, 2017, discusses justice, violence, patriarchy, and compassion, the critical importance of healing, and how to redefine resistance.
Protocols for Common Injuries from Police Weapons—A guide for street medics responding to non-lethal police munitions and chemical weapons
Appendix III: Using a Tourniquet
- Locate the wound.
- Apply tourniquet, over clothes if wound is clearly on an arm or leg and you can see a lot of blood.
- Make sure the red tip is pointing towards the heart. Place the tourniquet as high as possible. If the wound is below a knee or elbow, place the tourniquet just above the joint.
- Pull tail tight. Tighten the strap as tight as you can.
- Turn the windlass until the flow of blood stops.
- Mark the time.
Keep talking to the person you are treating.
![]()

Appendix IV: Building an Individual First Aid Kit (IFAK)
IFAK Build—Current lowest price per kit: $95.25, not including tax, shipping, or a bag or pouch for the kit. Here are the recommended contents, with links to sources:
- CAT Gen 7 (1) $30/each: available from NAR, Chinook, Rescue Essentials
- ETD (2) 4” flat, $7 each here
- Chest seal (2) Hyfin twin pack, $15/pair here
- Hemostatic gauze (1)—your options include ChitoGauze z-fold, 3”x4yd, $32/each (on sale) here, Celox rapid Z-fold, 3”x5’; you may need medical authorization to purchase. $34 each here, and QuikClot combat gauze z-fold, 3”x4yd, $43 each here
- Sharpie (1) Staples 12 pack, $8/12 on sale (.66/each) here
- Gloves (2 pair) Nitrile exam gloves size L, $13/100 ($.52/kit) here
- Shears (1) 7.5” stainless Shears, $3 each here
- Zipper bag for gloves (1) “sandwich size”, $3.50/50 ($.07/each) here
“Packing” means applying internal direct pressure to a severed vessel by creating pressure on that vessel with gauze, filling the wound with more gauze, holding direct pressure when the wound is filled, and finishing it with a pressure dressing. ↩
In this case, if someone has been shot, the hospital assumes that they may still be a target and aims to reduce the possibility of continued harm. ↩